
Archived Newsletter Re-Post.
The AOX Newsletter • January 2024 #4
It never fails. Ever.
I’m in the middle of an extremely difficult case and all the torque I can muster up on a particular implant is 25 N-cm. My composite torque is adequate, so I move forward with abutment placement in order to load.
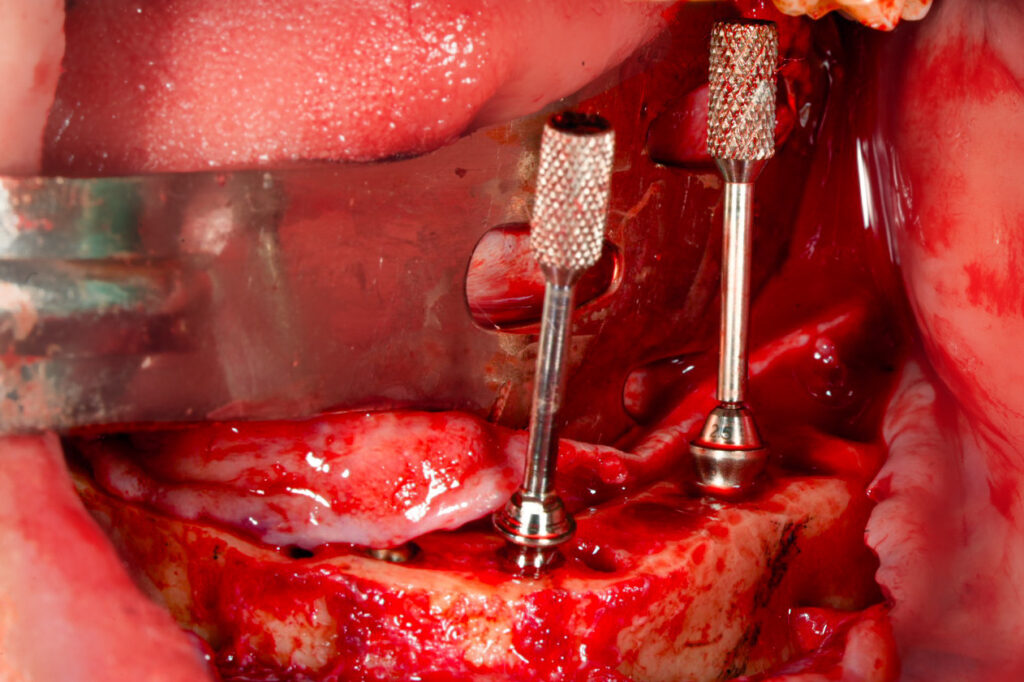
After verifying abutment angulation, I start to remove the abutment guide pins to begin placing healing caps and closing.
But wait! Ahhhhh?! Of course the 25 N-cm implant guide pin is on sooooo tight and will not come off?!
Why is it always the low torque implant that seems to have a guide pin that is stuck! This is the one implant I do not want to be messing with or putting excess force on!?
What now???
Well… Here are 3 steps I take to protect a low torque implant when removing an abutment guide pin that is “stuck”.
1. Hold the abutment with a small rongeur or hemostat.
- This prevents any rotation of the low torque implant when notable rotational force is applied to the guide pin.
- I hold the abutment and my assistant will loosen the guide pin.
2. For exceptionally tight guide pins, hold the abutment with a small rongeur or hemostat and utilize a lever arm to loosen the pin.
- As mentioned above, rotational forces are prevented by stabilization with a rongeur or hemostat.
- However, in this truly “stuck” scenario, I hold the abutment and have my assistant utilize a needle driver at a 90 degree angle to the guide pin to act as a lever arm. A rotational force is applied to the pin in order to loosen it.
- Ensure you maintain the 90 degree path. If you apply force at an off angle you can break the guide pin off in the abutment.
- If a fracture of the guide pin does actually occur – don’t stress – just switch out to a new abutment.
3. Loosen all abutment guide pins slightly, before placement in the mouth.
- I finally outsmarted that pesky pin. The easiest way to solve this problem is simply to prevent it in the first place.
- I now have my assistant loosen each guide pin before handing them to me. After loosening the pins, they are re-tightened, but only to a true, gentle “finger tight” torque. This ensures the guide pins can easily be removed on a low torque implant without the fear of rotating the implant itself.
Hope this helps when you’re feeling stuck…
Matthew Krieger DMD
“It’s the little details that are vital. Little things make big things happen.”
John Wooden
Q & A with Dr. K

“What is your drilling protocol? Do you under-prep your osteotomies?”
For a routine case, with average bone, I perform the following drilling sequence *for the Neodent Helix implant.
Maxilla: Prepare to a 3.5mm width. Place a 4.0mm width implant.
Posterior Mandible: Prepare to a 4.0mm width – but only extend the drill half the length of the osteotomy. Place a 4.0mm width imlpant.
Anterior Mandible: Prepare to a 4.0mm width – the entire length of the osteotomy. Place a 4.0mm width implant.
This typically generates torque in the range of 45-60+ N-cm.
Archived newsletters are released on a delayed timeline, a few months after the original publication. If you would like to receive these newsletters in real time please sign up here.